Diabetes is a chronic condition characterized by high levels of sugar (glucose) in the blood. The two types of diabetes are referred to as type 1 (insulin dependent) and type 2 (non-insulin dependent). Symptoms of diabetes include increased urine output, thirst, hunger, and fatigue. Treatment of diabetes depends on the type.
What is Diabetes?
Diabetes is a disease that occurs when your blood glucose, also called blood sugar, is too high. Blood glucose is your main source of energy and comes from the food you eat. Insulin, a hormone made by the pancreas, helps glucose from food get into your cells to be used for energy. Sometimes your body doesn’t make enough—or any—insulin or doesn’t use insulin well. Glucose then stays in your blood and doesn’t reach your cells.
Over time, having too much glucose in your blood can cause health problems. Although diabetes has no cure, you can take steps to manage your diabetes and stay healthy.
Sometimes people call diabetes “a touch of sugar” or “borderline diabetes.” These terms suggest that someone doesn’t really have diabetes or has a less serious case, but every case of diabetes is serious.
What are the different types of diabetes?
The most common types of diabetes are type 1, type 2, and gestational diabetes.
Type 1 diabetes
If you have type 1 diabetes, your body does not make insulin. Your immune system attacks and destroys the cells in your pancreas that make insulin. Type 1 diabetes is usually diagnosed in children and young adults, although it can appear at any age. People with type 1 diabetes need to take insulin every day to stay alive.
Type 2 diabetes
If you have type 2 diabetes, your body does not make or use insulin well. You can develop type 2 diabetes at any age, even during childhood. However, this type of diabetes occurs most often in middle-aged and older people. Type 2 is the most common type of diabetes.
Gestational diabetes
Gestational diabetes develops in some women when they are pregnant. Most of the time, this type of diabetes goes away after the baby is born. However, if you’ve had gestational diabetes, you have a greater chance of developing type 2 diabetes later in life. Sometimes diabetes diagnosed during pregnancy is actually type 2 diabetes.
Other types of diabetes
Less common types include monogenic diabetes, which is an inherited form of diabetes, and cystic fibrosis-related diabetes .
How common is diabetes?
As of 2015, 30.3 million people in the United States, or 9.4 percent of the population, had diabetes. More than 1 in 4 of them didn’t know they had the disease. Diabetes affects 1 in 4 people over the age of 65. About 90-95 percent of cases in adults are type 2 diabetes.1
Who is more likely to develop type 2 diabetes?
You are more likely to develop type 2 diabetes if you are age 45 or older, have a family history of diabetes, or are overweight. Physical inactivity, race, and certain health problems such as high blood pressure also affect your chance of developing type 2 diabetes. You are also more likely to develop type 2 diabetes if you have prediabetes or had gestational diabetes when you were pregnant. Learn more about risk factors for type 2 diabetes.
What health problems can people with diabetes develop?
Over time, high blood glucose leads to problems such as
heart disease
stroke
kidney disease
eye problems
dental disease
nerve damage
foot problems
You can take steps to lower your chances of developing these diabetes-related health problems.
Type 1 Diabetes
What is type 1 diabetes?
Diabetes occurs when your blood glucose, also called blood sugar, is too high. Blood glucose is your main source of energy and comes mainly from the food you eat. Insulin, a hormone made by the pancreas, helps the glucose in your blood get into your cells to be used for energy. Another hormone, glucagon, works with insulin to control blood glucose levels.
In most people with type 1 diabetes, the body’s immune system, which normally fights infection, attacks and destroys the cells in the pancreas that make insulin. As a result, your pancreas stops making insulin. Without insulin, glucose can’t get into your cells and your blood glucose rises above normal. People with type 1 diabetes need to take insulin every day to stay alive.
People with type 1 diabetes need to take insulin every day.
Who is more likely to develop type 1 diabetes?
Type 1 diabetes typically occurs in children and young adults, although it can appear at any age. Having a parent or sibling with the disease may increase your chance of developing type 1 diabetes. In the United States, about 5 percent of people with diabetes have type 1.1
What are the symptoms of type 1 diabetes?
Symptoms of type 1 diabetes are serious and usually happen quickly, over a few days to weeks. Symptoms can include
increased thirst and urination
increased hunger
blurred vision
fatigue
unexplained weight loss
Sometimes the first symptoms of type 1 diabetes are signs of a life-threatening condition called diabetic ketoacidosis (DKA) . Some symptoms of DKA include
DKA is serious and dangerous. If you or your child have symptoms of DKA, contact your health care professional right away, or go to the nearest hospital emergency room.
What causes type 1 diabetes?
Experts think type 1 diabetes is caused by genes and factors in the environment, such as viruses, that might trigger the disease. Researchers are working to pinpoint the causes of type 1 diabetes through studies such as TrialNet.
How do health care professionals diagnose type 1 diabetes?
Health care professionals usually test people for type 1 diabetes if they have clear-cut diabetes symptoms. Health care professionals most often use the random plasma glucose (RPG) test to diagnose type 1 diabetes. This blood test measures your blood glucose level at a single point in time. Sometimes health professionals also use the A1C blood test to find out how long someone has had high blood glucose.
Even though these tests can confirm that you have diabetes, they can’t identify what type you have. Treatment depends on the type of diabetes, so knowing whether you have type 1 or type 2 is important.
To find out if your diabetes is type 1, your health care professional may test your blood for certain autoantibodies. Autoantibodies are antibodies that attack your healthy tissues and cells by mistake. The presence of certain types of autoantibodies is common in type 1 but not in type 2 diabetes.
Because type 1 diabetes can run in families, your health care professional can test your family members for autoantibodies. Type 1 diabetes TrialNet, an international research network, also offers autoantibody testing to family members of people diagnosed with the disease. The presence of autoantibodies, even without diabetes symptoms, means the family member is more likely to develop type 1 diabetes. If you have a brother or sister, child, or parent with type 1 diabetes, you may want to get an autoantibody test. People age 20 or younger who have a cousin, aunt, uncle, niece, nephew, grandparent, or half-sibling with type 1 diabetes also may want to get tested.
What medicines do I need to treat my type 1 diabetes?
If you have type 1 diabetes, you must take insulin because your body no longer makes this hormone. Different types of insulin start to work at different speeds, and the effects of each last a different length of time. You may need to use more than one type. You can take insulin a number of ways. Common options include a needle and syringe, insulin pen, or insulin pump.
Some people who have trouble reaching their blood glucose targets with insulin alone also might need to take another type of diabetes medicine that works with insulin, such as pramlintide . Pramlintide, given by injection, helps keep blood glucose levels from going too high after eating. Few people with type 1 diabetes take pramlintide, however. The NIH has recently funded a large research study to test use of pramlintide along with insulin and glucagon in people with type 1 diabetes. Another diabetes medicine, metformin, may help decrease the amount of insulin you need to take, but more studies are needed to confirm this. Reseachers are also studying other diabetes pills that people with type 1 diabetes might take along with insulin.
Hypoglycemia, or low blood sugar, can occur if you take insulin but don’t match your dose with your food or physical activity. Severe hypoglycemia can be dangerous and needs to be treated right away. Learn more about hypoglycemia and how to prevent or treat it.
How else can I manage type 1 diabetes?
Along with insulin and any other medicines you use, you can manage your diabetes by taking care of yourself each day. Following your diabetes meal plan, being physically active, and checking your blood glucose often are some of the ways you can take care of yourself. Work with your health care team to come up with a diabetes care plan that works for you. If you are planning a pregnancy with diabetes, try to get your blood glucose levels in your target range before you get pregnant.
Do I have other treatment options for my type 1 diabetes?
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) has played an important role in developing “artificial pancreas” technology. An artificial pancreas replaces manual blood glucose testing and the use of insulin shots. A single system monitors blood glucose levels around the clock and provides insulin or a combination of insulin and glucagon automatically. The system can also be monitored remotely, for example by parents or medical staff.
In 2016, the U.S. Food and Drug Administration approved a type of artificial pancreas system called a hybrid closed-loop system. This system tests your glucose level every 5 minutes throughout the day and night through a continuous glucose monitor, and automatically gives you the right amount of basal insulin, a long-atcing insulin, through a separate insulin pump. You still need to manually adjust the amount of insulin the pump delivers at mealtimes and when you need a correction dose. You also will need to test your blood with a glucose meter several times a day. Talk with your health care provider about whether this system might be right for you.
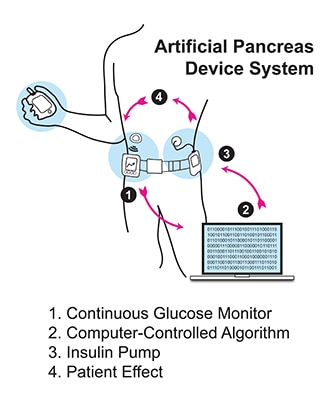
The illustration below shows the parts of a type of artificial pancreas system.
An artificial pancreas system uses a continuous glucose monitor, an insulin pump, and a control algorithm to give you the right amount of basal insulin.
The continuous glucose monitor sends information through a software program called a control algorithm. Based on your glucose level, the algorithm tells the insulin pump how much insulin to deliver. The software program could be installed on the pump or another device such as a cell phone or computer.
Starting in late 2016 and early 2017, the NIDDK has funded several important studies on different types of artificial pancreas devices to better help people with type 1 diabetes manage their disease. The devices may also help people with type 2 diabetes and gestational diabetes.
NIDDK is also supporting research into pancreatic islet transplantation—an experimental treatment for hard-to-control type 1 diabetes. Pancreatic islets are clusters of cells in the pancreas that make insulin. Type 1 diabetes attacks these cells. A pancreatic islet transplant replaces destroyed islets with new ones that make and release insulin. This procedure takes islets from the pancreas of an organ donor and transfers them to a person with type 1 diabetes. Because researchers are still studying pancreatic islet transplantation, the procedure is only available to people enrolled in a study. Learn more about islet transplantation studies.
What health problems can people with type 1 diabetes develop?
Over time, high blood glucose leads to problems such as
heart disease
stroke
kidney disease
eye problems
dental disease
nerve damage
foot problems
depression
sleep apnea
If you have type 1 diabetes, you can help prevent or delay the health problems of diabetes by managing your blood glucose, blood pressure, and cholesterol, and following your self-care plan.
Can I lower my chance of developing type 1 diabetes?
At this time, type 1 diabetes can’t be prevented. However, through studies such as TrialNet, researchers are working to identify possible ways to prevent or slow down the disease.
Type 2 Diabetes
What is type 2 diabetes?
Type 2 diabetes, the most common type of diabetes, is a disease that occurs when your blood glucose, also called blood sugar, is too high. Blood glucose is your main source of energy and comes mainly from the food you eat. Insulin, a hormone made by the pancreas, helps glucose get into your cells to be used for energy. In type 2 diabetes, your body doesn’t make enough insulin or doesn’t use insulin well. Too much glucose then stays in your blood, and not enough reaches your cells.
The good news is that you can take steps to prevent or delay the development of type 2 diabetes.
Who is more likely to develop type 2 diabetes?
You can develop type 2 diabetes at any age, even during childhood. However, type 2 diabetes occurs most often in middle-aged and older people. You are more likely to develop type 2 diabetes if you are age 45 or older, have a family history of diabetes, or are overweight or obese. Diabetes is more common in people who are African American, Hispanic/Latino, American Indian, Asian American, or Pacific Islander.
Physical inactivity and certain health problems such as high blood pressure affect your chances of developing type 2 diabetes. You are also more likely to develop type 2 diabetes if you have prediabetes or had gestational diabetes when you were pregnant. Learn more about risk factors for type 2 diabetes.
Type 2 diabetes occurs most often in middle-aged and older people.
What are the symptoms of diabetes?
Symptoms of diabetes include
increased thirst and urination
increased hunger
feeling tired
blurred vision
numbness or tingling in the feet or hands
sores that do not heal
unexplained weight loss
Symptoms of type 2 diabetes often develop slowly—over the course of several years—and can be so mild that you might not even notice them. Many people have no symptoms. Some people do not find out they have the disease until they have diabetes-related health problems, such as blurred vision or heart disease.
What causes type 2 diabetes?
Type 2 diabetes is caused by several factors, including
overweight and obesity
not being physically active
insulin resistance
genes
Learn more about the causes of type 2 diabetes.
How do health care professionals diagnose type 2 diabetes?
Your health care professional can diagnose type 2 diabetes based on blood tests. Learn more about blood tests for diabetes and what the results mean.
How can I manage my type 2 diabetes?
Managing your blood glucose, blood pressure, and cholesterol, and quitting smoking if you smoke, are important ways to manage your type 2 diabetes. Lifestyle changes that include planning healthy meals, limiting calories if you are overweight, and being physically active are also part of managing your diabetes. So is taking any prescribed medicines. Work with your health care team to create a diabetes care plan that works for you.
Following your meal plan helps you manage your diabetes.
What medicines do I need to treat my type 2 diabetes?
Along with following your diabetes care plan, you may need diabetes medicines, which may include pills or medicines you inject under your skin, such as insulin. Over time, you may need more than one diabetes medicine to manage your blood glucose. Even if you don’t take insulin, you may need it at special times, such as during pregnancy or if you are in the hospital. You also may need medicines for high blood pressure, high cholesterol, or other conditions.
Learn more about medicines, insulin, and other diabetes treatments.
What health problems can people with diabetes develop?
Following a good diabetes care plan can help protect against many diabetes-related health problems. However, if not managed, diabetes can lead to problems such as
heart disease and stroke
nerve damage
kidney disease
foot problems
eye disease
gum disease and other dental problems
sexual and bladder problems
Many people with type 2 diabetes also have nonalcoholic fatty liver disease (NAFLD). Losing weight if you are overweight or obese can improve NAFLD. Diabetes is also linked to other health problems such as sleep apnea, depression, some types of cancer, and dementia .
You can take steps to lower your chances of developing these diabetes-related health problems.
How can I lower my chances of developing type 2 diabetes?
Research such as the Diabetes Prevention Program , sponsored by the National Institutes of Health, has shown that you can take steps to reduce your chances of developing type 2 diabetes if you have risk factors for the disease. Here are some things you can do to lower your risk:
Lose weight if you are overweight, and keep it off. You may be able to prevent or delay diabetes by losing 5 to 7 percent of your current weight.1 For instance, if you weigh 200 pounds, your goal would be to lose about 10 to 14 pounds.
Move more. Get at least 30 minutes of physical activity, such as walking, at least 5 days a week. If you have not been active, talk with your health care professional about which activities are best. Start slowly and build up to your goal.
Eat healthy foods. Eat smaller portions to reduce the amount of calories you eat each day and help you lose weight. Choosing foods with less fat is another way to reduce calories. Drink water instead of sweetened beverages.
Ask your health care team what other changes you can make to prevent or delay type 2 diabetes.
Most often, your best chance for preventing type 2 diabetes is to make lifestyle changes that work for you long term. Get started with Your Game Plan to Prevent Type 2 Diabetes.
Insulin Resistance & Prediabetes
Insulin resistance and prediabetes occur when your body doesn’t use insulin well.
What is insulin?
Insulin is a hormone made by the pancreas that helps glucose in your blood enter cells in your muscle, fat, and liver, where it’s used for energy. Glucose comes from the food you eat. The liver also makes glucose in times of need, such as when you’re fasting. When blood glucose, also called blood sugar, levels rise after you eat, your pancreas releases insulin into the blood. Insulin then lowers blood glucose to keep it in the normal range.
What is insulin resistance?
Insulin resistance is when cells in your muscles, fat, and liver don’t respond well to insulin and can’t easily take up glucose from your blood. As a result, your pancreas makes more insulin to help glucose enter your cells. As long as your pancreas can make enough insulin to overcome your cells’ weak response to insulin, your blood glucose levels will stay in the healthy range.
What is prediabetes?
Prediabetes means your blood glucose levels are higher than normal but not high enough to be diagnosed as diabetes. Prediabetes usually occurs in people who already have some insulin resistance or whose beta cells in the pancreas aren’t making enough insulin to keep blood glucose in the normal range. Without enough insulin, extra glucose stays in your bloodstream rather than entering your cells. Over time, you could develop type 2 diabetes.
How common is prediabetes?
More than 84 million people ages 18 and older have prediabetes in the United States.1 That’s about 1 out of every 3 adults.
Who is more likely to develop insulin resistance or prediabetes?
People who have genetic or lifestyle risk factors are more likely to develop insulin resistance or prediabetes. Risk factors include
overweight or obesity
age 45 or older
a parent, brother, or sister with diabetes
African American, Alaska Native, American Indian, Asian American, Hispanic/Latino, Native Hawaiian, or Pacific Islander American ethnicity
physical inactivity
health conditions such as high blood pressure and abnormal cholesterol levels
a history of gestational diabetes
a history of heart disease or stroke
polycystic ovary syndrome, also called PCOS
People who have metabolic syndrome—a combination of high blood pressure, abnormal cholesterol levels, and large waist size—are more likely to have prediabetes.
Along with these risk factors, other things that may contribute to insulin resistance include
certain medicines, such as glucocorticoids , some antipsychotics , and some medicines for HIV
hormonal disorders, such as Cushing’s syndrome and acromegaly
Although you can’t change risk factors such as family history, age, or ethnicity, you can change lifestyle risk factors around eating, physical activity, and weight. These lifestyle changes can lower your chances of developing insulin resistance or prediabetes.
Being overweight or having obesity are risk factors for developing insulin resistance or prediabetes.
What causes insulin resistance and prediabetes?
Researchers don’t fully understand what causes insulin resistance and prediabetes, but they think excess weight and lack of physical activity are major factors.
Excess weight
Experts believe obesity, especially too much fat in the abdomen and around the organs, called visceral fat, is a main cause of insulin resistance. A waist measurement of 40 inches or more for men and 35 inches or more for women is linked to insulin resistance. This is true even if your body mass index (BMI) falls within the normal range. However, research has shown that Asian Americans may have an increased risk for insulin resistance even without a high BMI.
Researchers used to think that fat tissue was only for energy storage. However, studies have shown that belly fat makes hormones and other substances that can contribute to chronic, or long-lasting, inflammation in the body. Inflammation may play a role in insulin resistance, type 2 diabetes, and cardiovascular disease.
Excess weight may lead to insulin resistance, which in turn may play a part in the development of fatty liver disease.
Physical inactivity
Not getting enough physical activity is linked to insulin resistance and prediabetes. Regular physical activity causes changes in your body that make it better able to keep your blood glucose levels in balance.
What are the symptoms of insulin resistance and prediabetes?
Insulin resistance and prediabetes usually have no symptoms. Some people with prediabetes may have darkened skin in the armpit or on the back and sides of the neck, a condition called acanthosis nigricans. Many small skin growths called skin tags often appear in these same areas.
Even though blood glucose levels are not high enough to cause symptoms for most people, a few research studies have shown that some people with prediabetes may already have early changes in their eyes that can lead to retinopathy. This problem more often occurs in people with diabetes.
How do doctors diagnose insulin resistance and prediabetes?
Doctors use blood tests to find out if someone has prediabetes, but they don’t usually test for insulin resistance. The most accurate test for insulin resistance is complicated and used mostly for research.
Doctors use blood tests to find out if someone has prediabetes.
Doctors most often use the fasting plasma glucose (FPG) test or the A1C test to diagnose prediabetes. Less often, doctors use the oral glucose tolerance test (OGTT), which is more expensive and not as easy to give.
The A1C test reflects your average blood glucose over the past 3 months. The FPG and OGTT show your blood glucose level at the time of the test. The A1C test is not as sensitive as the other tests. In some people, it may miss prediabetes that the OGTT could catch. The OGTT can identify how your body handles glucose after a meal—often before your fasting blood glucose level becomes abnormal. Often doctors use the OGTT to check for gestational diabetes, a type of diabetes that develops during pregnancy.
People with prediabetes have up to a 50 percent chance of developing diabetes over the next 5 to 10 years. You can take steps to manage your prediabetes and prevent type 2 diabetes.
The following test results show Prediabetes2
A1C—5.7 to 6.4 percent
FPG—100 to 125 mg/dL (milligrams per deciliter)
OGTT—140 to 199 mg/dL
You should be tested for prediabetes if you are overweight or have obesity and have one or more other risk factors for diabetes, or if your parents, siblings, or children have type 2 diabetes. Even if you don’t have risk factors, you should start getting tested once you reach age 45.
If the results are normal but you have other risk factors for diabetes, you should be retested at least every 3 years.2
How can I prevent or reverse insulin resistance and prediabetes?
Physical activity and losing weight if you need to may help your body respond better to insulin. Taking small steps, such as eating healthier foods and moving more to lose weight, can help reverse insulin resistance and prevent or delay type 2 diabetes in people with prediabetes.
Physical activity can help prevent or reverse insulin resistance and prediabetes.
The National Institutes of Health-funded research study, the Diabetes Prevention Program(DPP), showed that for people at high risk of developing diabetes, losing 5 to 7 percent of their starting weight helped reduce their chance of developing the disease.3 That’s 10 to 14 pounds for someone who weighs 200 pounds. People in the study lost weight by changing their diet and being more physically active.
The DPP also showed that taking metformin , a medicine used to treat diabetes, could delay diabetes. Metformin worked best for women with a history of gestational diabetes, younger adults, and people with obesity. Ask your doctor if metformin might be right for you.
Making a plan, tracking your progress, and getting support from your health care professional, family, and friends can help you make lifestyle changes that may prevent or reverse insulin resistance and prediabetes. You may be able to take part in a lifestyle change program as part of the National Diabetes Prevention Program.
Clinical Trials
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions.
What are clinical trials, and are they right for you?
Clinical trials are part of clinical research and at the heart of all medical advances. Clinical trials look at new ways to prevent, detect, or treat disease. Researchers also use clinical trials to look at other aspects of care, such as improving the quality of life for people with chronic illnesses. Find out if clinical trials are right for you .
What clinical trials are open?
Clinical trials that are currently open and are recruiting can be viewed at www.ClinicalTrials.gov.
Gestational Diabetes
Definition & Facts
Gestational diabetes is a type of diabetes that occurs only during pregnancy. Gestational diabetes can cause health problems in both mother and baby. Managing your diabetes can help protect you and your baby.
Symptoms & Causes
Gestational diabetes often has no symptoms, or they may be mild, such as being thirstier than normal or having to urinate more often. Gestational diabetes is sometimes related to the hormonal changes of pregnancy that make your body less able to use insulin. Genes and extra weight may also play a role.
Tests & Diagnosis
Your doctor will test you for gestational diabetes between 24 and 28 weeks of pregnancy. Tests include the glucose challenge test and the oral glucose tolerance test (OGTT). If the results of the glucose challenge test show high blood glucose, you will return for an OGTT test to confirm the diagnosis of gestational diabetes.
Management & Treatment
Managing gestational diabetes includes following a healthy eating plan and being physically active. If your eating plan and physical activity aren’t enough to keep your blood glucose in your target range, you may need insulin.
Prevention
You can lower your chance of getting gestational diabetes by losing extra weight before you get pregnant if you are overweight. Being physically active before and during pregnancy also may help prevent gestational diabetes.
After Your Baby is Born
If you had gestational diabetes, you are more likely to develop type 2 diabetes. Your child is more likely to become obese or develop type 2 diabetes. You may be able to lower your and your child’s chances of developing these problems by reaching a healthy weight, making healthy food choices, and being physically active.
Related Conditions & Diseases
Health Tips for Pregnant Women
Type 2 Diabetes
Clinical Trials
The NIDDK and other components of the National Institutes of Health (NIH) support and conduct research into many diseases and conditions.
View clinical trials that are currently recruiting volunteers .
Additional Languages
This content is also available in:
Spanish
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings through its clearinghouses and education programs to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
The most common forms of diabetes, type 1 and type 2, are polygenic, meaning they are related to a change, or defect, in multiple genes. Environmental factors, such as obesity in the case of type 2 diabetes, also play a part in the development of polygenic forms of diabetes. Polygenic forms of diabetes often run in families. Doctors diagnose polygenic forms of diabetes by testing blood glucose, also known as blood sugar, in individuals with risk factors or symptoms of diabetes.
Genes provide the instructions for making proteins within the cell. If a gene has a change or mutation, the protein may not function properly. Genetic mutations that cause diabetes affect proteins that play a role in the ability of the body to produce insulin or in the ability of insulin to lower blood glucose. People typically have two copies of most genes, with one gene inherited from each parent.
What are monogenic forms of diabetes?
Some rare forms of diabetes result from mutations or changes in a single gene and are called monogenic. In the United States, monogenic forms of diabetes account for about 1 to 4 percent of all cases of diabetes.1,2,3,4 In most cases of monogenic diabetes, the gene mutation is inherited from one or both parents. Sometimes the gene mutation develops spontaneously, meaning that the mutation is not carried by either of the parents. Most mutations that cause monogenic diabetes reduce the body’s ability to produce insulin, a protein produced in the pancreas that helps the body use glucose for energy.
Neonatal diabetes mellitus (NDM) and maturity-onset diabetes of the young (MODY) are the two main forms of monogenic diabetes. NDM occurs in newborns and young infants. MODY is much more common than NDM and usually first occurs in adolescence or early adulthood.
Most cases of monogenic diabetes are incorrectly diagnosed. For example, when high blood glucose is first detected in adulthood, type 2 diabetes is often diagnosed instead of monogenic diabetes. If your health care provider thinks you might have monogenic diabetes, genetic testing may be needed to diagnose it and to identify which type. Testing of other family members may also be indicated to determine whether they are at risk for or already have a monogenic form of diabetes that is passed down from generation to generation. Some monogenic forms of diabetes can be treated with oral diabetes medicines (pills), while other forms require insulin injections. A correct diagnosis allows for proper treatment and can lead to better glucose control and improved health in the long term.
What is neonatal diabetes mellitus (NDM)?
NDM is a monogenic form of diabetes that occurs in the first 6 to 12 months of life. NDM is a rare condition accounting for up to 1 in 400,000 infants in the United States.4 Infants with NDM do not produce enough insulin, leading to an increase in blood glucose. NDM is often mistaken for type 1 diabetes, but type 1 diabetes is very rarely seen before 6 months of age. Diabetes that occurs in the first 6 months of life almost always has a genetic cause. Researchers have identified a number of specific genes and mutations that can cause NDM. In about half of those with NDM, the condition is lifelong and is called permanent neonatal diabetes mellitus (PNDM). In the rest of those with NDM, the condition is transient, or temporary, and disappears during infancy but can reappear later in life. This type of NDM is called transient neonatal diabetes mellitus (TNDM).
Clinical features of NDM depend on the gene mutations a person has. Signs of NDM include frequent urination, rapid breathing, and dehydration.5 NDM can be diagnosed by finding elevated levels of glucose in blood or urine. The lack of insulin may cause the body to produce chemicals called ketones, resulting in a potentially life-threatening condition called diabetic ketoacidosis. Most fetuses with NDM do not grow well in the womb, and newborns with NDM are much smaller than those of the same gestational age, a condition called intrauterine growth restriction. After birth, some infants fail to gain weight and grow as rapidly as other infants of the same age and sex. Appropriate therapy may improve and normalize growth and development.
What is maturity onset diabetes of the young (MODY)?
MODY is a monogenic form of diabetes that usually first occurs during adolescence or early adulthood. MODY accounts for up to 2 percent of all cases of diabetes in the United States in people ages 20 and younger.3
A number of different gene mutations have been shown to cause MODY, all of which limit the ability of the pancreas to produce insulin. This leads to high blood glucose levels and, in time, may damage body tissues, particularly the eyes, kidneys, nerves, and blood vessels.
Clinical features of MODY depend on the gene mutations a person has. People with certain types of mutations may have slightly high blood sugar levels that remain stable throughout life, have mild or no symptoms of diabetes, and do not develop any long-term complications. Their high blood glucose levels may only be discovered during routine blood tests. However, other mutations require specific treatment with either insulin or a type of oral diabetes medication called sulfonylureas.
MODY may be confused with type 1 or type 2 diabetes. In the past, people with MODY have generally not been overweight or obese, or have other risk factors for type 2 diabetes, such as high blood pressure or abnormal blood fat levels. However, as more people in the United States become overweight or obese, people with MODY may also be overweight or obese.
Although both type 2 diabetes and MODY can run in families, people with MODY typically have a family history of diabetes in multiple successive generations, meaning MODY is present in a grandparent, a parent, and a child.
How is monogenic diabetes diagnosed?
Genetic testing can diagnose most forms of monogenic diabetes. A correct diagnosis with proper treatment should lead to better glucose control and improved health in the long term.
Genetic testing is recommended if 6
diabetes is diagnosed within the first 6 months of age
diabetes is diagnosed in children and young adults, particularly those with a strong family history of diabetes, who do not have typical features of type 1 or type 2 diabetes, such as the presence of diabetes-related autoantibodies, obesity, and other metabolic features
a person has stable, mild fasting hyperglycemia, especially if obesity is not present
If you think that you or a member of your family may have a monogenic form of diabetes, talk to your doctor.
What do I need to know about genetic testing and counseling?
Genetic testing for monogenic diabetes involves providing a blood or saliva sample from which DNA is isolated. The DNA is analyzed for changes in the genes that cause monogenic diabetes. Genetic testing is done by specialized labs.
Abnormal results can determine the gene responsible for diabetes in a particular individual or show whether someone is likely to develop a monogenic form of diabetes in the future. Genetic testing can be helpful in selecting the most appropriate treatment for individuals with monogenic diabetes. Testing is also important in planning for pregnancy and to understand the risk of having a child with monogenic diabetes if you, your partner, or your family members have monogenic diabetes.
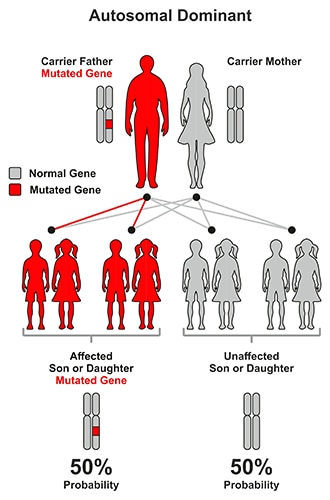
Most forms of NDM and MODY are caused by autosomal dominant mutations, meaning that the condition can be passed on to children when only one parent carries or has the disease gene. With dominant mutations, a parent who carries the gene has a 50 percent chance of having an affected child with monogenic diabetes.
In most forms of MODY, a parent with MODY has a 50 percent chance of having a child with the disease.
In contrast, with autosomal recessive disease, a mutation must be inherited from both parents. In this instance, a child has a 25 percent chance of having monogenic diabetes.
For recessive forms of monogenic diabetes, testing can indicate whether parents or siblings without disease are carriers for recessive genetic conditions that could be inherited by their children.
While not as common, it is possible to inherit mutations from the mother only (X-linked mutations). Also not as common are mutations that occur spontaneously.
When both parents carry autosomal recessive mutations, a child has a 25 percent chance of having (or being affected by) the disease.
More information about the genes that cause NDM and MODY, the types of mutations responsible for the disease (autosomal dominant, autosomal recessive, X-linked, etc.), and clinical features is provided in the American Diabetes Association Standards of Medical Care in Diabetes.
If you suspect that you or a member of your family may have a monogenic form of diabetes, you should seek help from health care professionals—physicians and genetic counselors—who have specialized knowledge and experience in this area. They can determine whether genetic testing is appropriate; select the genetic tests that should be performed; and provide information about the basic principles of genetics, genetic testing options, and confidentiality issues. They also can review the test results with the patient or parent after testing, make recommendations about how to proceed, and discuss testing options for other family members.
How is monogenic diabetes treated and managed?
Treatment varies depending on the specific genetic mutation that has caused a person’s monogenic diabetes. People with certain forms of MODY and NDM can be treated with a sulfonylurea, an oral diabetes medicine that helps the body release more insulin into the blood. Other people may need insulin injections. Some people with MODY may not need medications and are able to manage their diabetes with lifestyle changes alone, which include physical activity and healthy food choices. Your physician and diabetes care team will work with you to develop a plan to treat and manage your diabetes based on the results of genetic testing.
Clinical Trials
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) and other components of the National Institutes of Health (NIH) conduct and support research into many diseases and conditions.
What are clinical trials, and are they right for you?
Clinical trials are part of clinical research and at the heart of all medical advances. Clinical trials look at new ways to prevent, detect, or treat disease. Researchers also use clinical trials to look at other aspects of care, such as improving the quality of life for people with chronic illnesses. Find out if clinical trials are right for you .
اس قبیلے کا دنیا سے کو ئی رابطہ نہیں، یہ لوگ کیا کھاتے ہیں اور کیسے رہتے ہیں؟ تفصیلات ایسی کہ آپ سوچ بھی نہیں سکتے برازیلیا(مانیٹرنگ ڈیسک) برازیل میں واقع ایمازون کے جنگلات میں بسنے والے قبیلے، جو بیرونی دنیا سے الگ تھلگ رہتے تھے، جنگل کٹ جانے کے باعث اسی جگہ پر بسائے جانے والے دیہاتوں میں رہنے لگے ہیں اور باقی دنیا کے ساتھ ان کا رابطہ ہو چکا ہے لیکن اب بھی کئی ایسی قبیلے ہیں جو باقی ماندہ جنگل میں رہائش پذیر ہیں اور ان کا اب بھی بیرونی دنیا سے کوئی رابطہ نہیں ہے۔ میل آن لائن کے مطابق ان میں ایک قبیلے کا نام Awaیا Guajaہے، جسے سب سے زیادہ معدومی کے خطرے سے دوچار قبیلہ قرار دیا جا چکا ہے۔ اب اس قبیلے کے افراد کی تعداد صرف 600رہ گئی ہے جو ایسی زبان بولتے ہیں جو باقی دنیا میں کسی کی سمجھ میں نہیں آتی۔ کچھ عرصہ قبل فوٹوگرافر ڈومینیکو پگلیسے کشتی کا طویل سفر کرکے اس قبیلے کے رہنے کی جگہ کے قریب پہنچا اور دور سے ہی ان کی تصاویر بنا دنیا کوان کے رہن سہن سے متعارف کروایا۔ اس قبیلے کے لوگ اب بھی خونخوار جنگلی جانوروں کو پالتو جانوروں کے طور پر پالتے ہیں۔ یہ لوگ ان جانوروں کو اس و...
یہ معجزاتی سفر آپ کی عظمت ورفعت پر ایک روشن دلیل ، انسانیت کی معراج اور بندگی کا سب سے بلند و بالا اعزاز ہے خاتم الانبیاء،سرورِ کونین، حضرت محمد مصطفیٰ ﷺ کے معجزات میں سے ایک عظیم معجزہ معراج النبیﷺ ہے۔’’ معراج‘‘ عروج سے مشتق ہے، عروج کے معنیٰ ہیں بلندی پر جانا۔خاتم النبیین حضرت محمد ﷺ سے قبل جتنے انبیائے کرامؑ تشریف لائے، یہ بلندی اللہ تعالیٰ نے سب کو عطا فرمائی، لیکن دیگر انبیائے کرامؑ کی معراج اور آنحضرت ﷺ کی معراج میں نمایاں فرق یہ ہے کہ دیگر تمام انبیائے کرامؑ کو یہ عظمت و بلندی اللہ تعالیٰ نے فرش پر عطا فرمائی،جب کہ حضور اکرم ﷺ کو یہ عظمت و رفعت اور بلندی اللہ تعالیٰ نے عرش پر عطا فرمائی۔یہ ایک روشن حقیقت ہے کہ نبی اکرمﷺ کے اعلان نبوت سے پہلے کے چالیس سالہ دور میں کفار مکہ متفقہ طور پر محمد ابن عبداللہ کی حیثیت سے آپﷺ کو صادق اور امین کے لقب سے پکارتے تھے۔ دیانت کے حوالے سے آپ کے پاس بلا جھجک، بلا خوف و خطر اپنی امانتیں رکھواتے تھے،لیکن جیسے ہی آپ ﷺ نے اپنی عمر کے چالیس سال مکمل فرمائے۔ آپﷺ نے بحیثیت محمد رسول اللہﷺ اعلان نبوت فرمایا اور کلمۂ حق کے قبول کرنے کی دعو...
Supreme Court to hear APS attack case on Oct 5 More than 140 people, most of them students, were martyred in the terrorist attack in Dec 2014. ISLAMABAD After a longstanding demand of the victim’s parents to conduct a judicial inquiry into the 2014 APS massacre, the Surpeme Court of Pakistan has fixed October 5 as the date for hearing of the suo moto notice. A three-member bench headed by Chief Justice Saqib Nisar will hear the case. Notices have also been sent to the attorney general and advocate general of Khyber Pakhtunkhwa among others. It may be mentioned here that Chief Justice Saqib Nisar had had taken a suo motu notice of the matter in April this year when parents of some victims approached him while he was hearing other cases in Peshawar. In May, the apex court had ordered probe into the APS massacre through a judicial commission comprising a judge of the Peshawar High Court (PHC). On December 16, 2014, the horrific terr...










Comments
Post a Comment